Narratives of Health Protection in Families with a Late-Onset Kidney Disease: Re-Defining Governmentality and Responsibility for Health in the Era of the 'New' Genetics
by Lucy Brindle
University of Southampton
Sociological Research Online 14(5)23
<http://www.socresonline.org.uk/14/5/23.html>
doi:10.5153/sro.2060
Received: 23 Jun 2009 Accepted: 22 Nov 2009 Published: 30 Nov 2009
Abstract
Genetic medical technologies have increased the possibilities for detecting future illness in those who appear healthy and asymptomatic. These developments broaden the scope of medicine, complicating distinctions between health, illness and disease. Genetic counselling practice extends health promotion seeking to 'inform' individuals of their own risks so that they can minimise possible negative implications for their own lives (Lupton 1995). An extension of disease prevention has been associated with a shift in health such that health is no longer a given but has to be achieved by individuals. While post-structuralist accounts have positioned health promotion as part of an increasing self-surveillance of health, they have rarely based these accounts on empirical studies of individuals' experiences. This paper explores how 'early' diagnosis positions people as 'at-risk'. Findings inform narratives of social change centred on the individualisation of health, the extension of self-surveillance and the blurring of boundaries between health and disease. Narrative accounts from interviews and observations of clinical consultations with 18 adults who had been told that they had inherited a late onset, degenerative kidney disease (Autosomal Dominant Polycystic Kidney Disease) are used to explore how individuals discursively achieve health and appropriate health protection. This analysis challenges the idea that knowledge of genetic aetiology will reduce individual responsibility for health. Rather than a grand shift to a continuum of health and the disappearance of 'old' binaries, these participants appear to use the health/disease dualism to re-position themselves with respect to risk on a moment-by-moment basis.
Keywords: Governmentality; Risk; New Genetics; Responsibility for Health; Agency; Normality; Early Diagnosis
Responsibility for health
1.1From a perspective within which health and illness are not properties of individuals to be treated as given but are claims to be sustained 'against the background of competing moral demands' (Radley and Billig, 1996), health status is always potentially fluid and negotiable. However the increasing use of assessment of risks to health, and pre-symptomatic diagnosis, also provides the possibility for health status to be negotiated around the likelihood and location in time of future events. This paper took, as its point of departure, theory proposing that within local practices of self, individuals are increasingly being formulated as having responsibility for the reduction of their own health risks (Lupton, 1993) and an interest in the implications of having a diagnosis of ADPKD, a late-onset hereditary kidney disease, for the positioning of selves and others as responsible for health.1.2 Within a discourse of risk associated with the development of public health, risk becomes a consequence of 'life style' choices made by the individual (Lupton, 1993). The risk discourse relating to public health can be described as an extension of the idea, characteristic of a 'risk society' (Beck, 1992), that individuals should attempt to protect themselves against possible future mishaps and plan for the future. The extension of this discourse, and the development of public disease prevention practices, have been associated with a shift in health such that health is no longer a given but has to be achieved by individuals (Lupton, 1995). The increasing use of risk assessments and provision of diagnoses which predict future ill health might be expected to further disturb distinctions between health and disease, provide ambiguous health identities and re-define responsibilities for health.
1.3 A Foucauldian 'governmentality' narrative, outlining a process of normalisation and surveillance/self surveillance of health, has provided counter narratives to rational accounts of the development of public health and thus responsibilities for health. However, even though governance as a theoretical framework has been used to account for individuals' involvement in health promotion practices, there have been few empirical studies of governance that have addressed individuals' experiences of disease prevention (Howson, 1999).
1.4 Foucauldian accounts of the movement of disease into the dispensary or social sphere, have also informed accounts of more general change in the social construction of health. For example, an increase in chronic illness in an ageing population and a shift in the 'medical gaze' has been associated with a blurring of boundaries between health and disease. A shift has been described from the body, where disease was located as a discrete phenomenon, to the social sphere following the second world war (Arney and Bergen, 1984; Nettleton, 2006; Armstrong, 1983). These changes extended the realm of medicine to include lifestyle and brought about a move from binary divisions of health and disease to a continuum of health. Nettleton has argued:
'thus there has been a shift from the biological anatomy of the body to its political anatomy. With this change in the structures of medical institutions, the dichotomies between health and disease, sane and insane, young and old, normal and abnormal, have become blurred. Instead of being placed on either side of these binary divides, bodies are placed on a continuum.' (2006: 120)
1.5 Whereas accounts of social change such as these might be used to 'predict' how technical developments within the field of genetics will impact upon responsibilities for health, Tilly (1994; 1999) has argued for understandings of social change to be built upon historically grounded (social constructionist) analyses. He proposes that by fixing account of change to historically grounded generalisations it is possible to confront inadequate and over-generalised accounts of social change.
1.6 In 'The Trouble with Stories' Tilly proposes a route from participants' stories to explanations of social processes that would involve a social constructionist analyses of storytelling itself, thereby creating 'compelling' explanations for:
" the stories that participants in social processes tell about what is happening to themselves or others.." (1999: 267)On the premise that story telling is fundamental to social construction and everyday life, he proposes that telling "the true story of how storytelling arises and how it affects our conduct of social life" (1999: 268) will provide more adequate accounts of social processes per se.
1.7 Although proposing a social constructionist analysis, Tilly provides a realist representation of the relationship between narrative and social processes: he argues that the causal processes within social processes are usually indirect, accumulative, interactive, unintended, collective, environmentally mediated, and in contradiction to the causal structure constructed within most every day (and some social science) explanations of social life. An implication of this incongruence between social processes and every day social explanation (which he refers to as 'standard stories') is that the accurate explanation of social processes will require explanations in 'non-standard' story form.
1.8 Tilly's realist account of cause and effect within social processes might be criticised for not going as far as deconstructing the notion of causality itself. However, his work provides a framework within which to delineate a relationship between accounts produced by participants and large scale social processes which carries significant de and re-constructive potential. Furthermore, by treating analysts' accounts as socially constructed and therefore an object of analyses, he introduces reflexivity into an empirically grounded analysis of social process which promotes an evaluation of alternative explanations on the basis of their relative adequacy and plausibility.
1.9 This article describes research involving participants with a late onset hereditary kidney disease, ADPKD (Autosomal Dominant Polycystic Kidney Disease). By making the types of comparisons, generalisations and distinctions, proposed by Tilly, between small stories told in the research interview and genetic counselling consultation, it was possible to critique and refine contemporary narratives of large scale change in the social organisation of responsibilities for health.
The Research
2.1 ADPKD is a late onset, degenerative kidney disease characterised by a gradual decline in kidney function resulting in end stage kidney failure (ESRF). Adults with ADPKD are usually diagnosed in their 30s and 40s and have an average age of entry into ESRF of 57 years. The age of onset of symptoms is highly variable but there is likely to be a period of 'declining health' prior to ESRF (Wilkie et al, 1985).2.2 When this research was conducted (1994-1997) genetic diagnostic techniques for ADPKD had recently been developed, so that in addition to diagnosis by ultrasound (which was age dependent) DNA tests could indicate carrier status and thus likelihood of developing the disease in the future, regardless of age (Gabow, 1994). A pilot study had been set up in the UK regional genetics service in which this research took place to explore the implications of extending genetic testing for ADPKD to children. However, the possibilities for childhood testing that this pilot offered generated limited interest from the parents who were invited to participate. This article discusses data from a larger study of the social construction of parents' experiences of living with ADPKD and views on testing in childhood, which was developed in response to parents' lack of interest in testing children, and which formed my PhD research.
2.3 Participants and Study Recruitment: Participants (adults with a diagnosis of ADPKD and children under the age of 19) were recruited from two sources, a research register and a research clinic providing genetic counselling and childhood testing for ADPKD, both located within a regional NHS genetics service within the UK. All participants were initially contacted by a clinical geneticist and then recruited by the non-clinical PhD student (LB). My status within the clinic was one of research assistant and observer and it was explained to potential participants that I did not have a professional role within the genetic service. The numbers of potential participants were low and consequently sampling was opportunistic rather than a purposive. Eighteen adults agreed to participate in the study. Six of these participants and their families also attended the genetic counselling clinic and agreed to have their clinical consultations tape-recorded. Whilst all research clinic attendees approached to take part in this study agreed to do so, response rates were not available for those contacted by letter.
2.4 Most participants (fifteen) had not yet reached end stage renal failure (ESRF). Of the three participants who had reached ESRF, two had received transplants and one was receiving renal replacement therapy at the time of interview. Participants received an annual outpatient appointment at which kidney function and blood pressure were assessed. Some also received treatment for hypertension. As the decline in kidney function approached levels requiring dialysis, outpatient appointments occurred more frequently until those affected reached a designated threshold at which renal replacement therapy was provided. Therefore most were involved with practices of surveillance. Although not raised by the researcher, actions taken by the participant to avoid ill health were a common theme in interviews, and this is the focus of the analysis presented in this paper.
2.5 Interviews and Analysis: The research outlined in this article uses an ethnomethodological discourse analysis to explore governance from 'the underside'. The research interview and the clinical consultation are treated as two sites at which social relationships built the social world. Therefore the 'veracity' of accounts generated within the interview or consultation is not an issue.
2.6 Interviews were carried out in the participant's own home and on occasions also involved the participant's partner and/or children. Some participants were interviewed on more than one occasion: those attending the research clinic, where possible, were also interviewed before the consultation. Open questions were used in interviews to generate accounts of experiences of living with a diagnosis of ADPKD. Questions included those about experiences of family history prior to diagnosis, the experience of 'having' ADPKD and the implications of diagnosis for the participant. All questions were treated as constructive in them selves and included in analyses. A range of probes and follow-up questions were also used to further explore participants' constructive and narrative resources (discussed in greater detail in Brindle, 2000).
2.7 Interviews and research clinic consultations with study participants were audio-recorded and transcribed verbatim. If family members were present in the interview this is indicated at the start of the extract. Material which might identify the participant or family members has been removed from the extract and the sex of some family members has been disguised. Square brackets and a descriptive label are used to represent any material that had been omitted. Round brackets are used to indicate inaudible speech. The study was granted NHS REC approval.
2.8 Questions designed to elicit accounts of participants' experiences and views, would be expected to invoke evaluative accounts of personal lives and hence, loosely defined, narration. Whereas narrative might be defined merely on the basis of its difference to discourse, 'as an entity that is distinguishable from the surrounding discourse and (which) has a beginning, a middle and an end.' (Hyden, 1997: 50), notions of temporality and emplotment frequently feature in researchers' definitions. For example, Maines has described 3 common assumptions within the narrative approach. These are that events are selected from the past for purpose of commentary, temporally ordered and emploted in a way which confers "structure, meaning and context" on events (1993: 21). The analytic process presented in this article does not attempt to isolate narratives as objects per se. Whilst recognising narration as ubiquitous social process, the analysis of which would be expected to feature within a social constructionist analysis of the research interview, I set out to explore social processes (including narrative) as the 'contingent, changing products of interaction' (Tilly 1994: 264). That is, the analytical approach incorporates ethnomethodological concerns that much narrative analysis has neglected variation in situations and interactional contexts, and therefore, has also neglected the implications of this variation for the constitution of stories. For example, Schegloff (2006) argues that by taking narrative rather than talk-in-interaction as the focus of analysis, the consequences of context, and hence the situated production of narrative is pushed to the background.
2.9 Whereas sociologists have recognised a need to treat narrative as a social phenomena rather than a privileged account of a private experience or inner world (Atkinson, 1997; Atkinson and Delamont, 2006), this might be achieved without any tight definition of narrative. For example Atkinson proposed:
'What is important is the general recognition that there exist as social phenomena an array of spoken and written forms that provide culturally appropriate ways in which personal experience is shared, knowledge is transmitted, memories are enacted and testimony is constructed.' (2006: xxi)
2.10 There are clearly parallel tensions in discourse and narrative analyses between discourse/narrative as a cultural artefact and discourse/narrative as talk-in-interaction/action (e.g. Wetherell; Schegloff: 1998; Atkinson and Delamont, 1997). The analytic approach taken here edges toward the latter, that is an ethnomethodological analysis, whilst also incorporating a sense of discourse as cultural resource, informed by a post-structuralist reading of discourse (Wetherell 1998; Davies & Harre 1990; Foucault 1971; Derrida 1973 & 1976) (For a further discussion see Brindle, 2000).
2.11 Hence the study presented in this article uses an ethnomethodological discourse analysis to explore how the lifestyles of those with ADPKD, health protection and 'taking care of health' were socially constructed and narrated by participants or clinicians. The analytic process involves focussing on variation and sequence within accounts (Sacks 1995; Schegloff 1972 & 1992; Potter et al. 1990), the rhetorical organisation of accounts and hence 'counter-narrative' and thus explores situated social action.
2.12 The extracts presented here are taken from interviews with four of the participants and from a genetic counselling consultation with one of these adults. This focus on a small number of case-studies demonstrates the variation and sequencing within accounts (Sacks, 1984) which informed more generalised explanations accounting for 'systematic variations' in the construction and the organisation of discourse within the larger data set (Potter et al, 1990: 208).
2.13 The analysis is organised under three headings: 'Risk and normality as resources for self protection', 'Counter-narratives: the rhetorical organisation of appropriate lifestyles' and 'Agency achieves health'. These headings are not used to typify accounts but to draw attention to particular organisations of discourse and social action.
Risk and normality as resources for self protection
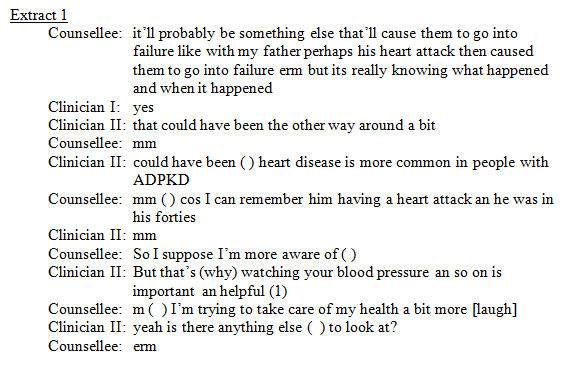
3.1 One of the ways in which appropriate health protection was formulated was by attending to an individual's risk status relative to those without ADPKD. A formulation of relative risk, in which risks to health were constructed as the binary of either different or not to those without ADPKD, was used by clinicians and affected adults to establish the importance of taking actions that might be viewed as health protective. In the analytic account that follows, alternative formulations of at-risk groupings are identified in order to highlight the constructed nature of the normality/difference distinction and to demonstrate how this formulation is used to achieve appropriate health protection.3.2 In the extract 1, below, taken from a genetic counselling consultation, the relationship between having ADPKD and a heart attack suffered by the counsellee's father, is being discussed.
|
3.3 In the second and third lines of the extract the counsellee refers to her father's heart attack as a cause of his kidney failure. However this proposed independence of her father's heart attack from ADPKD is countered in the clinician's next turn. The counsellee is located as at higher than usual risk of heart attack by the statement that heart disease is more common in those with ADPKD. Thus, a contrast is made between those who have and those who do not have ADPKD and those with ADPKD are assessed as being at greater risk in contrast to population risk. The use of this categorisation allows a qualitative state of greater risk and therefore 'at-risk' to be applied to ADPKD. No indication is given of either the likelihood of a person with ADPKD having a heart attack or of the strength of association between ADPKD and heart disease.
3.4 The greater likelihood of heart attack with ADPKD is presented as a reason for a particular importance of protecting health through 'watching your blood pressure and so on'. Heart attacks and self surveillance are therefore made of particular relevance to her. In the ordering of these statements health protection follows as a suitable response to this assessment of risk. The possibility of risk reduction becomes almost a component of a statement of higher risk. Therefore, following a positioning (Davies and Harre, 1990) of the counsellee as having greater risk, she is then re-positioned as being able to adjust that risk. Control and responsibility is placed back with the individual.
3.5 The counsellee responds to the possibility of taking a specific action to protect health by referring to her more general lifestyle behaviour. In stating 'I'm trying to take care of my health a bit more' the counsellee takes up a position of having a personal approach to health protection. Thus, in response to the formulation of blood pressure as a preventable risk to health, risk reduction is taken up as a moral issue for her own management. The statement 'looking after my health a bit more' suggests a change in activity corresponding to a current health status and therefore as taking actions that are (more) appropriate since her diagnosis.
3.6 Genetic consultations, by presenting genetic risks as manageable and encouraging self-surveillance, have been viewed as offering (or 'promising') control over uncertainties (Hallowell,1999). Hallowell goes on to argue that by labelling individuals as 'at-risk', 'and presenting genetic risks as manageable, genetic counselling implicitly places individuals under an obligation to attempt to modify these risks' (Hallowell,1999: 599). Discourses of risk and prevention which render controllable uncertain futures, can be understood as tools of rationalisation and the modern project (Game, 1991). Of analytic concern is the implications of these statements, rather than the intentions or motivations of the social actors themselves, that is, the counsellee is located as an agent of her own future health.
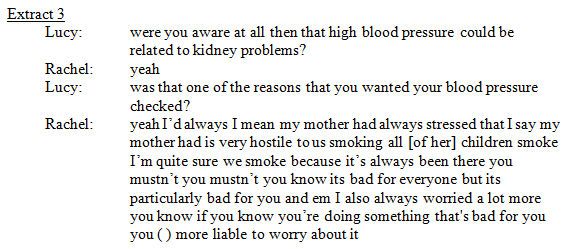
3.7 A binary formulation of relative risk involving difference or not to others was also used by those with ADPKD. For example, Rachel counters a formulation of smoking behaviour as less appropriate for those with ADPKD, by reformulating the dangers from smoking in terms of risks for all those who smoke relative to risks for those who don't. She follows a request to smoke during the research interview with a comment on the position of others to her smoking since her diagnosis:

|
3.8 Rachel responds to the stated disapproval of smoking since her diagnosis, by normalising the risk to her health from smoking. The implication that smoking is less appropriate because of having ADPKD is countered by reformulating the higher risk category so it also includes those without ADPKD. She provides an account in which she isn't different from others on the basis of having ADPKD. Of interest is that the participant does not justify smoking by constructing the risks posed as normal or reasonable but by placing herself within the same risk grouping as those who don't have ADPKD. However, the same participant also formulates smoking as posing dangers that justify concerns about health. This formulation of risk occurs within an account explaining why she requested to have her blood pressure checked in her early twenties:
|
3.9 In the last three lines of the extract Rachel suggests that she was worried because she knew she was doing something that was bad for her. The formulation of this statement in terms of knowing (rather than thinking) 'you're doing something that's bad for you' constructs the harmful nature of smoking as factual. Of interest in these two accounts is the contextual construction of smoking as 'bad for you' in explaining concern about blood pressure but also as bad for all smokers in justifying smoking behaviour. Constructions of risks within a normality-difference dualism could be used as a resource to achieve appropriate health protection without constructing either the danger to health or the likelihood of such a danger.
3.10 This analysis of Rachel's accounts of her smoking behaviour demonstrates that rather than being able to identify and isolate a conceptualisation of a risk to health from smoking which is assumed to underlie the participant's own explanations for her own behaviour, constructions of risk obtain their meaning from their location in accounts. The construction of risks to health occurs in accounts performing other social actions such as explanations of requests for medical checks, justifying lifestyles or formulating what is necessary and appropriate health protective behaviour for individuals. That is, the analysis provides a critique of a prevalent explanation in which 'risk perceptions' function as 'mental predictates' (Tilly, 2004) and hence account for participant's 'sense-making' about 'health behaviour'.
3.11 By drawing upon Foucauldian notions of disciplinary power and practices of self, disease prevention practices have been portrayed as practices of surveillance (Armstrong, 1995, Nettleton 1992). According to Foucault, discipline operates through a combination of observation and normalising judgement (Foucault, 1977; Dreyfus and Rabinow, 1982). Normalisation, as a practice which compares individuals to others, involves the production of difference in relation to sameness. However, such normalising practices can be understood as both totalising and individualising (Game, 1991). The construction by participants of their risks as normal could be understood as resistance to their positioning as having different responsibilities for health. Therefore a discourse of normalisation was used to resist its own potential positioning of subjects as 'outside the norm'.
3.12 Despite the possibilities for resistance from within a discourse of normalisation, those with a diagnosis of ADPKD can become accountable for that which they know, that which they tell others and how they protect their own health. For example, Rachel despite constructing ADPKD as 'just another illness' and everybody else as having 'things in their family that's likely to carry them off', made herself accountable for her smoking behaviour and for her desire not to know about her children's ADPKD status (Brindle, 2000). In both of these cases she managed issues of responsibility from within a positioning of being different.
3.13 An orientation to the relevance of difference for the social organisation and constitution of health, appropriate lifestyles and responsibilities for health, was also apparent in the rhetorical organisation of narratives to counter a need to change 'normal' lifestyles after diagnosis.
Counter-narratives: The rhetorical organisation of appropriate lifestyles
4.1 Accounts of lifestyles and lifestyle advice were often rhetorically organised to counter a need to make changes to 'normal lifestyles' following a diagnosis of ADPKD. The use of 'having nothing wrong', to legitimate the continuance of previous lifestyles following diagnosis, reflects the existence of associations between 'sickness' and responsibilities for the adjustment of behaviour, including lifestyles. Having nothing wrong (or 'it' having not happened') was established in these accounts by referring to having normal kidney functioning or 'normal' blood pressure. These arguments could be made despite reported symptoms of ADPKD.4.2 This use of health/disease and normality/abnormality dualities to manage responsibilities for health provides little support for a general shift from binary divisions of health and disease to a continuum of health as has been proposed by Nettleton (2006). Furthermore, the same participant would use multiple constructions of the meaning of having a gene. Such multiplicity fits more closely with a fragmented, indexical and moment-by moment conceptualisation of health, rather than a representation of health as a point on a continuum. Adults with ADPKD would variably describe themselves as 'knowing that they have it', as 'just having it' since diagnosis, as 'not yet having developed it' and even as 'not having it' (Brindle, 2000). Whereas accounting for genetic variation in terms of 'having' a disease is made possible by a discourse of disease that locates disease as a physical abnormality within the body (Foucault, 1973), this 'accumulated culture' (Tilly, 1999: 268) does not appear to determine the construction of personal health.
4.3 Despite much variation in the way that a person's health status might be constructed, the rhetorical organisation of accounts to counter a need to change lifestyles following diagnosis, displayed systematic features. Protecting health and maintaining normal lifestyles appeared to be orientated to by participants as possibly dilemmatic. That is dilemmatic, in the sense of Billig et al's (1988) notion of 'ideological dilemmas', wherein one position invokes a counter-position. Arguments for 'living a normal life' were usually accompanied by formulations of lifestyles that accomplished responsible self-protection and demonstrated a willingness to make adjustments to lifestyle, if necessary, to protect health.
4.4 Participants often referred to medical advice in their accounts of diagnosis but also drew attention to contradictions within and between diverse sources of lifestyle advice. In the following narrative account of a parent's response to the participant's diagnosis, a dilemma or tension between living a normal life and 'taking' care was voiced:

|
4.5 In this account health protection was formulated in terms of 'taking care', however, a tension between taking care and living normally was also apparent. By phrasing health protection in the terms of 'look(ing) after yourself', the advice given implies a need for positive action, rather than just restriction. This advice is immediately followed by a recounting of 'just live normally mind you' as a possible counter-position to the preceding statement.
4.6 Smoking was presented as 'the big thing' in another's account and cast doubt on through the lack of congruence between smoking behaviour and onset of 'it' in family members. Therefore, the veracity of this relationship was left in doubt. However, the participant ends this narrative by stating that he does not smoke anyway, and therefore is not placing himself at risk.
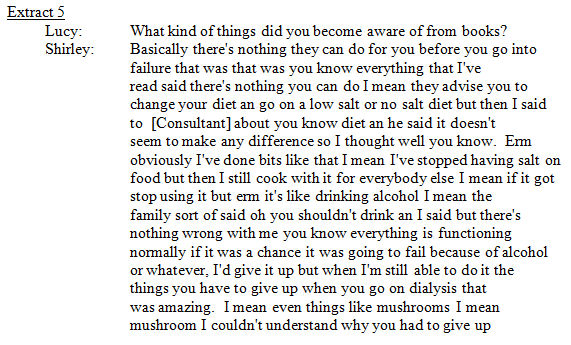
4.7 Reference to items of medical advice within accounts was often used to provide justification for particular lifestyles, or for not adjusting lifestyles following diagnosis. For example, within the following extract Shirley refers to the consultant's advice about adjusting salt intake. This is placed within an account of the participant's use of books as a source of information about ADPKD. Shirley begins by making a statement about the inability to prevent or treat the condition prior to kidney failure:
|
4.8 The statement 'there is nothing you can do' to prevent ADPKD is followed with advice from a textbook to 'go on a low salt diet'. The inclusion of this information then allows its exclusion through the opposing medical advice that 'it doesn't seem to make any difference' and therefore the maintenance of the position that there is no prevention. However, following on from this position, the participant states that 'erm obviously I've done bits like'. By stating that these actions were 'obviously' done, she is constructing herself as having no doubt that this is appropriate and that she is willing to take such actions. Shirley goes on to substantiate her willingness to 'do bits'. She says 'like that I mean I've stopped having salt on food '.
4.9 The suggestion that drinking is incongruent with 'having a disease' was responded to by stating that drinking is not a cause of kidney failure. However, the lack of a causal relationship was not used in isolation to justify drinking behaviour. 'Not being ill' also strengthened this position. The use of 'there's nothing wrong with me' as a resource in opposing the censoring of drinking makes sense within a discourse associating disease with restrictions on acceptable lifestyles. Despite opposing the possible association between having ADPKD and having 'something wrong', the use of comments such as 'obviously I've done bits like', suggests that the participant orientates to and makes herself accountable in relation to a position in which different responsibilities for health arise from a diagnosis.
4.10 The interviewee goes on to justify her lifestyle by emphasising the positive value in doing things while still able. Associations can be made with 'making the most of life' in contrast to failing to live while possible. The importance of quality of life is tied into this position by explicitly stating the pleasurable nature, and hence value of these activities: ' ...all the things I really enjoy out of life and I thought well when I can enjoy have them ..'
4.11 Therefore, in formulating appropriate health protective behaviour the interviewee manages responsibility for health by constructing herself as doing what is reasonable, but also adopts a position in which she argues for the importance of living fully. Responsible lifestyle behaviour is managed by referring to professional advice about the prevention of ADPKD, by constructing herself as taking action to protect health and by arguing that she is not, in fact, ill. The co-existence of the importance of 'living while able' reformulates the association between health and behaviour by making these activities a possibility provided by health rather than as implicated in future health.
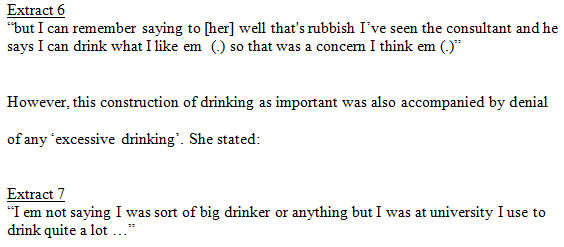
4.12 Medical advice was used in a number of narratives about lifestyle to support claims that there was no need to restrict lifestyle because of ADPKD. For example, Rachel, in an account of her concern at the time of diagnosis about being able to continue to drink alcohol, narrates an instance when a family member suggested that she would no longer be able to 'drink'. Rachel rejected this suggestion by referring to medical advice. She said:
|
4.13 The representation of her as drinking a lot but not excessively is made possible by constructing the behaviour as a type of behaviour normal for the context, that is, 'being at university', rather than being the problem of an individual. Rachel thereby formulates her lifestyle behaviour as reasonable at the time of diagnosis.
4.14 Within narratives about lifestyle, participants oriented to a positioning in which they might be expected to change their lifestyles following diagnosis. On occasions medical advice was used to provide a legitimate counter position to this possibility. However, participants were also able to contest items of medical advice and manage possibly conflicting information. A practice of 'lay epidemiology' (Davison et al, 1992) was apparent and those with ADPKD were also able to reformulate at risk groupings hence demonstrating the relativity of risk. Furthermore, participants tended to formulate them selves as exercising agency in health protection, rather than as dependent on singular sources of information or the direction of others. The selective use of medical advice regarding lifestyle, as a justificatory devise, might provide a means of managing the relativity of risk and the moral status of an individual's relationship with health within the social relationships which constitute our society.
4.15 Occasions on which lifestyle was raised but participants did not make themselves accountable for their own health included when questions were being asked of clinicians about the possible health protective qualities of changes in lifestyle or when changes in personal lifestyle resulting from kidney failure, symptoms of ADPKD or other life changes, were being discussed. Accounts that included arguments against childhood testing for ADPKD also demonstrated some differences to the accounts presented so far.
4.16 In the extracts discussed within which the participant's own health was the topic and participants continued 'normal lifestyles' after diagnosis, narratives negotiated the health protective nature of the participant's lifestyle and were more likely to appear dilemmatic, in that participants also demonstrated a willingness to take action to protect health. Participants on occasions would refer to an inability to prevent kidney failure or medical advice, but these positions were not used alone to formulate a lifestyle as appropriate. Participants also tended to construct themselves as exercising agency in practising appropriate health protection. In contrast, narratives about lifestyle which occurred as part of arguments against childhood testing demonstrated less complexity in the range of social actions being managed in relation to the participant's own health. Narratives about the participant's own lifestyle were used to demonstrate that it was not possible to make lifestyle changes that were preventative. Medical advice was often used to legitimise this position. However, parental agency tended not to feature in these narratives.
4.17 A reliance on arguments about prevention and medical advice to justify not testing children demonstrates parents' orientation to a narrative in which childhood testing might be justified if there were health benefits and to the medical profession as the legitimate holders of knowledge that might indicate a need to test children on health grounds. Furthermore, the presence of an agentic individual, taking control of their own health, in lifestyle narratives which occur within accounts for which the participant's own health is the topic, suggests a greater 'lay' responsibility for lifestyle decisions.
Agency achieves health
5.1 The presentation of an autonomous, self-regulated citizen, seeking to minimise their risks, provides support for the Foucauldian notion that individuals are involved in the self-surveillance of health:'A central aspect of governmentality in neo-liberal societies is the idealised figure of the autonomous, self-regulated citizen. Such individuals voluntarily seek to maximise their life opportunities and minimise the risks to which they are exposed. They police their own behaviour and need only guidance and advice from 'expert' knowledges to engage in activities that serve their best interests.' (LUPTON, 1999: 61)However, this analysis of lifestyle narratives suggests a further extension of the role of agency in health such that, within lifestyle narratives, agency might actually provide protection against disease.
5.2 The following case study presents a long extract in which explanations for health differences within a family (and hence a family epidemiology) was provided. The presentation and analysis of this long account enables a more detailed exploration of relations between the construction of agency, lifestyle and health.
5.3 The following extract displays similarities to previous extracts, in that the participant made herself accountable for her lifestyle on the basis of having a diagnosis of ADPKD. In this case the status of the participant's own lifestyle as both healthy and protective of health is formulated in relation to 'worse' cases. This comparison between lifestyles is managed through a formulation of individual differences in how family members responded to 'knowing' about diagnosis. Constructions of the moral and agentic status of lifestyle behaviour, following diagnosis, are used to formulate family members as having personal approaches to health protection (even before diagnosis) and to assess the healthiness of a person's lifestyle. Whether the appropriate lifestyle for a person with ADPKD was actively chosen by the individual, passively adopted or 'enforced' by external events is used as a resource to construct both current health and the health protective status of lifestyles. Therefore, rather than 'lifestyles' being assigned to pre-existing categories with respect to their healthiness or threats to future health, the formulation of lifestyles as health protective or not is dependent on the formulation of the individual as exercising agency in behaving responsibly.
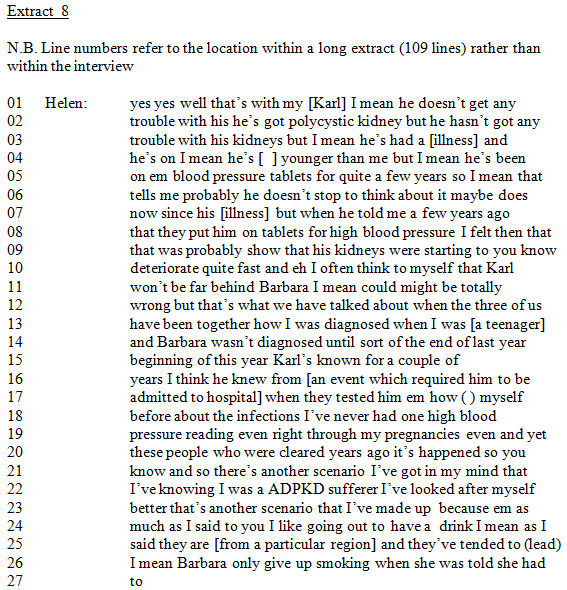
5.4 In the first section of the extract, below, the interviewee discusses her own and two other family members' health and 'stage' of ADPKD. Following the construction of her two family members' states of health as worse than her own, the participant explains these differences with reference to individual's lifestyles.
|
5.5 Following a discussion about the relationship between blood pressure and 'other complications' of ADPKD (not shown) Helen goes on to account for her relative, Karl's high blood pressure as signifying the rate of kidney deterioration. This is done in an account of her feelings at the time that Karl was prescribed tablets for hypertension. Following a statement in lines 2-3 that Karl did not actually have any problems with his kidneys, in lines 7-12 Helen talks about having 'felt' that his high blood pressure did signify his stage of kidney disease. She formulates high blood pressure as showing both rapid kidney deterioration and as signifying time to onset of kidney failure.
5.6 Prior to the statement relating Karl's high blood pressure to his stage of disease, Helen also says that despite Karl being younger than her he's both had a [illness event] and is on blood pressure tablets. By referring to age, these differences in state of health can be attributed to stage of disease as an independent phenomenon, rather than differences in age. This construction of Karl's stage of ADPKD as being particularly advanced makes possible a later construction of his disease as more advanced than her own. However the discursive production of disease stage is worked up gradually by attending to possible refutations and counter claims over a number of statements. The use of 'I felt' and 'thought', to construct Karl's state of health as Helen's own subjective position, avoids claiming the possession of legitimate knowledge regarding the state of this individual's kidneys, therefore making contestation of the account on grounds of validity more difficult.
5.7 The construction of family members as being at different stages of disease progression makes relevant an explanation for these differences. Differences in stage and rate of disease progression are also established by making relevant the location of diagnosis in the life course. Helen argues that the time between diagnosis and signs of kidney deterioration, differs for the three family members. By contrasting time of diagnosis with current state of health and by formulating the better state of health of those diagnosed earlier as a discrepancy, diagnosis as time of disease appearance is implied. This formulation of Helen as having slower progression is based on formulations of her as having both earlier appearance of 'disease' and later onset of signs of deterioration. An absence of high blood pressure readings, even in pregnancy, is used in contrast to the high blood pressure experienced by her relatives to present her health as better than other affected family members'. The mention of pregnancy as a time when women in general may be more likely to have hypertension but she did not, functions to further disassociate her from having a state of disease that shows itself in hypertension. Kidney infections in her late teens and early twenties are raised and exempted from the discussion of signs of illness. She says in lines 17-21:

|
5.8 A distinction is made between herself and her two family members for whom 'it's happened'. Barbara has already reached kidney failure but Karl was earlier described as not having 'any trouble with his kidneys'. Although what 'it' refers to is not made explicit, an anomaly between time of diagnosis and 'it' implies that 'it' is a sign of ADPKD onset. Therefore what is earlier established as a tentative possibility at this stage becomes ADPKD onset.
5.9 Once these differences have been established as independent of the teller, a possible explanation for them is formulated as a 'scenario I've got in my mind'. The use of 'scenario', might make this account more difficult to discredit on the basis that it claims invalid 'knowledge' rights as a causal explanation.
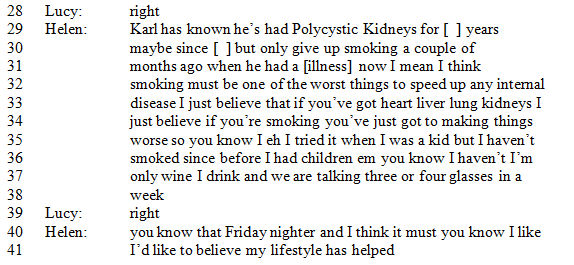
5.10 Knowledge of being an 'ADPKD sufferer' is presented as the reason for Helen having looked after her self better. Helen uses this 'scenario' as an explanation for [Barbara] (although older) being in kidney failure and [Karl] (younger) having ADPKD related health problems. However, in contrast to what might be expected, Helen does not then compare the period in her life when she knew she had ADPKD with the period in Barbara's and Karl's when they did not have this knowledge. Rather, Barbara and Karl are constructed as generally having different lifestyles and approaches to health protection than herself. Their lifestyles prior to diagnosis are not described in any detail but are established in relation to what her own is not. That she did 'look after herself better' is established over a number of sentences. Helen starts and ends this discussion of lifestyles with reference to her own lifestyle behaviour. She states:

|
5.11 Behaviour that might be classified as not health protective is raised as a prefix to and reference point for relatively worse behaviour. Her drinking behaviour is thereby excluded from the type of behaviour she is referring to in Barbara and Karl's case. Following a construction of smoking as stupid for those with ADPKD, Helen's own smoking behaviour during her life is located in a specific time period and made a distant activity. That she 'tried it', rather than actually describing herself as smoking at that time, presents this as other than part of her lifestyle. Her drinking behaviour is also constructed as moderate.
5.12 A general orientation towards health and a 'type' of lifestyle is implied in the statement 'I mean they are [from a particular region] and they tended to lead'. However this type of lifestyle is not then elaborated by describing types or quantities of behaviour. Instead Helen goes on to construct them as having a general approach to health protection by either stating that they failed to change behaviours after diagnosis or that any behaviour change was not agentic. A lack of agency is implied by the statement that '[Barbara] only gave up smoking when she was told she had to'. The 'health protective' status of lifestyles is being formulated, not only on the basis of the type of lifestyle adopted, but also in relation to an individual's orientation or attitude to health protection. The individual is constructed as either self monitoring and taking control of their own health or alternatively, as only acting when not having any choice. A moral position around 'looking after yourself' is thereby created.
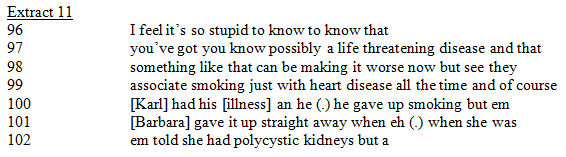
5.13 The use later on in the extract of alternative formulations of Barbara's cessation of smoking demonstrates the function-orientated nature of this construction. For example, when Helen is formulating the stupidity of Karl's behaviour in contrast to the behaviour of others she describes Barbara as having given 'it up straight away' (line 101):
|
Karl is constructed as continuing to smoke and therefore still failing to protect his health on knowing that he had ADPKD. This follows an earlier statement (lines 31-35) in which smoking was described as, 'one of the worst things to speed up any internal disease', and was therefore made a particularly risky activity for those with ADPKD.
5.14 In the intermediate section of the interaction (not shown the extract is presented in Brindle 2000) Helen establishes ADPKD as her reason for not smoking by refuting possible alternative explanations. She describes smoking as a desirable activity at the time. She says 'I quite envy people who could light up'. Therefore she constructs herself as actively and agentically avoiding harmful activities because she had ADPKD.
Summary of the use of agency as a resource
6.1 Helen produces an account in which she constructs her own state of health as better than her affected family members and provides explanations for these differences in terms of individual differences in approaches to health protection. An analysis of the discursive organisation of this account draws attention to how constructions of differences in health and differences in approaches to health protection are achieved. Agency and a person's response to 'knowing' they had ADPKD are used as resources to construct a person's health status and the health protective nature of their lifestyle. The agentic and health protective status of individuals' behaviour are established through the construction of self/other differences. Within this account Helen is producing subject positions and subjectivities in which she is agentic, takes responsibility for her own health and is currently healthy, but has normal interests in social and lifestyle activities.6.2 The analysis presented is demonstrative of Tilly's (1994) claim that 'standard stories' construct causality as singular, direct and intentional and that a social constructionist analysis of how such construction occurs has the potential to illuminate the relationship between the discursive organisation of stories and the social action and social organisation of which they are part: in this case the relationship between discursive organisation and the constitution of agency as a cause of health. However, it is important to note that the use of agency to achieve health is not presented as a characteristic of 'lay' accounting in contrast to a 'scientific' approach to risk assessment.
6.3 The potential to use agency as a resource to discursively achieve health itself and to account for differences in health between individuals, provides support for the thesis that the political achievement of a relationship between lifestyle and health, associated with the development of health promotion, has extended the concept of health such that health no longer arises primarily from the body:
' for now, health is derived from its social, economic and cultural dimensions in an absolute and critical reversal of medicine's relation to the social body. Where, for medical science, the body of the patient acted as the prime source and object of health, for health promoters the wellness of individuals is a product of lifestyle. Far from a medicalisation of health, medicine is relegated to one structure among others from which a particular biographical 'wellbeing' is socially constructed.' (O'Brien, 1995: 193).
6.4 The narratives produced by those with ADPKD demonstrate a reflexive crafting of biographies in which individual volition and agentic 'self-care' produce wellness. This connection of agency with health might be explained, as O'Brien's account suggests, as a result of health promoters' positioning of individual wellness as a product of lifestyle and hence the de-differentiation of health into everyday life.
6.5 The social construction of 'biographical wellbeing' referred to by O'Brien has similarities with Beck and Gidden's conceptualisation of increasing individualisation in modern society, wherein individuals increasingly have to reflexively craft their own biographies. According to Beck, despite the construction of individuals 'through a complex discursive interplay which is much more open-ended than the functionalist role model would assume', the 'compulsion' to individualisation (Beck, 1994: 16) and hence displays of agency are not necessarily liberating in themselves. By drawing upon Beck's account, the relationship between agency and health might be explained within a more general grand narrative which depicts increasing individualisation as a product of social and economic change associated with a loss of traditional roles and certainties. Whereas the analyses described in this paper provided some support for the individualisation of lifestyle, an assumption that a notion of 'individualisation' might be extended to all areas of social life or to all actions in which participants are involved, is avoided. In doing so a concept of individuality as a 'mental predicate' (Tilly, 1994), an interpretation that might be applied to Beck's text, is unsupported by this analytic account.
The 'new genetics' and shifts in responsibility for health
7.1 Formulating the relationship between ill health and responsibility in terms of aetiology of disease has also led to the suggestion that the new genetics might absolve the individual of responsibility for lifestyle: 'When the cause of disease is genetic, emphasis to some extent shifts away from personal responsibility, at least in relation to the control of lifestyle factors' (Lupton, 2003: 101). Whereas Hallowell has suggested that an inability to blame inherited risk on external sources acts to emphasise responsibility for self-protection (Hallowell, 1999).7.2 This focus on the relationship between aetiology of disease and responsibility for health appears to obscure the concerns and orientations of the social actors themselves. An inability to ultimately prevent kidney failure did not absolve individuals of all responsibility for lifestyle, that is, they oriented to and rhetorically opposed the need to practise 'abnormally' restrictive lifestyles but narrated personal choices to adopt health protective lifestyles. Furthermore, medical advice included the values of self-surveillance 'keeping an eye on' and 'looking after' health. That is, despite genetic aetiology, participants might still be positioned as having accentuated responsibilities for health protection associated with a diagnosis of ADPKD. However, the proposal that an inability to attribute causation to the external world accentuates responsibility, was also not supported by this analysis. Discourses around which responsibilities were negotiated were those of difference or not to others, rather than the origin of dangers to health.
Discussion
8.1 Tilly has proposed fixing accounts of social change to historically grounded generalisations. By 'generalisation' Tilly meant statements attached to:'specific eras and parts of the world, specifying causes, involving variation from one instance to another, within their time-space limits' (1984: 60).
8.2 The account provided in this paper has been organised around an analysis of the local and situated production of responsibility for health and thus has provided a messy and more complex account of social changes in health than those provided by grand (and deterministic) narratives of individualisation, geneticisation, governmentality and stories of shifts to a continuum of health.
8.3 This study explored the social construction of responsibilities for health at two sites at which social relationships built the social world the research interview and a genetic counselling clinic. Further generalisation, and thus an enhanced understanding of the relations between the various social processes involved in the changing constitution of health, would involve a wider ranging series of comparisons between particular discursive contexts and institutional settings. For example, even though governance might appear to produce responsibilities which have wider reaching implications than the consideration of lifestyle, how and when this occurs for those with a diagnosis of ADPKD would require systematic exploration. To achieve the type of generalisations that Tilly has proposed, conditions for the individualisation of lifestyle and the implications of this process would require further exploration across a range of social interactions as would the veracity (or limits) of Beck's claim that individualisation is a more general phenomena. For example, the type of comparison made in this paper between the construction of lifestyle within arguments against childhood testing and within accounts where the participant's own health was the topic might be extended to other 'topics', social practices and settings.
8.4 What we have ended up with is a 'superior story' (Tilly, 1999) which might be crafted as such:
As medical technologies develop, our abilities to define abnormalities or 'differences' that have a relationship with future disease are likely to increase. Thus, the possibilities for the 'normalisation' of pathology are likely to increase within an ever broadening gaze that identifies an increasing number of individuals as having embodied signifiers of future ill health. The analysis presented in this paper suggests that increasing geneticisation will not necessarily increase personal responsibility for health in societies where governmentality provides 'being the same' as a counter-narrative to that of 'rational' disease prevention. However, neither is a relationship between 'cause' and responsibility, such that genetic aetiology reduces responsibility for health, or an assumption that the possibilities for resistance provided by the techniques of governance absolve individuals of responsibility for health, supported by participants' narratives. However, support is provided for an 'individualisation' (Beck, 1994) of lifestyle generally and for the relevance of diagnosis as a point at which lifestyle becomes the 'legitimate' business of others and around which individuals demonstrate the self-surveillance of health.
Conclusion
9.1 So we are left with a story of large scale social processes, which has involved a movement away from the 'relational story' (Tilly, 1999) that informed the analyses, that is, a story based in an emic approach which treats social systems as contingent, changing products of interaction. As Tilly pointed out, some stories are exclusive. Theories of governmentality and individualisation, for example, provide their own narratives formulating particular causal pathways. Within the governmentality narrative crafted by this article, the public practices involved in disease prevention still achieve particular responsibilities for health and thus, the situated social actions and interactions which constitute social life are muted. However, using 'small stories' about health protection told by those with ADPKD, to draw attention to the inadequacies of particular grand narratives about geneticisation, governmentality and shifts towards a continuum of health, produces, in Tilly's terms, a 'superior', albeit a more complex and therefore messier story about changes in responsibilities for health.
Acknowledgements
I would like to thank Dr Kate Verrier-Jones, Professor Angus Clarke and all those who participated for making this project a possibility. I would also like to thank the editor Liz Stanley, the anonymous referees and Professor Cathy Pope for their helpful comments on an earlier draft of this manuscript and Professors Srikant Sarangi and Roisin Pill for their encouragement.
References
ARMSTRONG, D. (1983) Political Anatomy of the Body: Medical Knowledge in Britain in the 20th Century. Cambridge: Cambridge University Press
ARMSTRONG, D. (1995) 'The rise of surveillance medicine', Sociology of Health and Illness, 17, 3, 383-404. [doi:10.1111/1467-9566.ep10933329]
ARNEY, W. R. and BERNARD, B. (1984) Medicine and the management of living: Taming the last great beast. London: University of Chicago Press.
ATKINSON, P. A. (1997) 'Narrative turn of blind alley?' Qualitative Health Research 7, 3, 325-344 [doi:10.1177/104973239700700302]
ATKINSON, P. A. and DELAMONT, S. (2006) 'Editors' Introduction: Narratives, Lives, Performances' In Narrative Methods: Volume I Sage Publications Ltd: London
BECK, U, (1992) Risk Society, Towards a New Modernity. Trans. M. Ritter London: Sage
BECK, U, (1994) 'The reinvention of Politics' In Beck, U., Giddens, A., and Lash, S., (editors) Reflexive Modernisation: Politics, Tradition and Aesthetics in the Modern Social Order. Oxford: Oxford University Press.
BILLIG, M., CONDOR, S., EDWARDS, D., GANE, M., MIDDLETON, D. and RADLEY, A. (1988) Ideological Dilemmas: A Social Psychology of Everyday Thinking. London: Sage.
BRINDLE, L. (2000), Formulating risk and normality: constructing experiences of having Autosomal Dominant Polycystic Kidney Disease. Unpublished PhD thesis. University of Wales College of Medicine.
DAVIES, B. and HARRE, R. (1990) 'Positioning: the discursive production of selves', Journal for the Theory of Social Behaviour, 20, 43-63. [doi:10.1111/j.1468-5914.1990.tb00174.x]
DAVISON, C. (1992) 'The limits of lifestyle: Reassessing 'Fatalism' in the Popular Culture of Illness Prevention', Social Science and Medicine, 6, 675-685. [doi:10.1016/0277-9536(92)90195-V]
DERRIDA, J. (1973) Writing and Difference. London: Routledge and Kegan Paul.
DREYFUS, H. and RABINOW, P. (1982) Michel Foucault: Beyond Structuralism and Hermeneutics. Brighton: Harvester Press.
FOUCAULT, M. (1971) 'Orders of Discourse' Social Science Information. 10, 7-30. [doi:10.1177/053901847101000201]
FOUCAULT, M. (1973) The Birth of the Clinic. London: Tavistock.
FOUCAULT, M. (1977) Discipline and Punish. London: Penguin.
GABOW, (1994) Assessing Genetic Risks: Implications for health and social policy. Washington: National Academy Press.
GAME, A. (1991) Undoing the social: Towards a deconstructive sociology. Milton Keynes: Open University Press.
HALLOWELL, N. (1999) 'Doing the right thing: genetic risk and responsibility', Sociology of Health and Illness, 21, 5, 597-621. [doi:10.1111/1467-9566.00175]
HOWSON, A. (1999) 'Cervical screening, compliance and moral obligation'. Sociology of Health & Illness, 21, 401-425. [doi:10.1111/1467-9566.00164]
HYDEN, L-C (1997) 'Illness and narrative' Sociology of Health & Illness 19, 1, 48-69.
LUPTON, D. (1993) 'Risk as Moral Danger: the social and political functions of risk discourse in public health', International Journal of Health Services Research, 23, 425-35.
LUPTON, D. (1995) The Imperative of Health: Public Health and the Regulated Body. London: Sage
LUPTON, D. (1999) Risk and sociocultural theory: New directions and perspectives. Cambridge: Cambridge University Press [doi:10.1017/CBO9780511520778]
LUPTON, D. (2003) Medicine as Culture. Sage Publications: London
MAINES, D. R. (1993) 'Narrative's Moment and Sociology's Phenomena: Towards a Narrative Sociology' Sociological Quarterly, 34, 1, 17-38. [doi:10.1111/j.1533-8525.1993.tb00128.x]
NETTLETON, S. (1992) Power, Pain and Dentistry. Buckingham: Open University Press.
NETTLETON, S. (2006) The Sociology of Health and Illness. Cambridge: Polity Press.
O'BRIEN, M. (1995) 'Health and Lifestyle: A Critical Mess?' In Bunton, R., Nettleton, S. and Burrows, R. (editors). The Sociology of Health Promotion: A critical analysis of lifestyle, consumerisn and risk. London: Routledge [doi:10.4324/9780203429495_chapter_15]
POTTER, J., WETHERELL, M., GILL, R. and EDWARDS, D. (1990) 'Discourse: noun, verb or social practice?' Philosophical Psychology, 3, 205-217. [doi:10.1080/09515089008572999]
RADLEY, A. and BILLIG, M. (1996) 'Accounts of Health and Illness: Dilemmas and representations'. Sociology of Health & Illness, 18, 220-240. [doi:10.1111/1467-9566.ep10934984]
SACKS, H. (1984) 'On Doing 'Being Ordinary' in Atkinson, J. M. and Heritage, J. (editors). Structures of Social Action: Studies in Conversation Analysis: Cambridge: Cambridge University Press.
SACKS, H. (1995) 'Lectures on conversation'. Jefferson G, (ed) Cambridge, MA: Blackwell
SCHEGLOFF, E. A. (1972) Notes on a conversation practice: formulating place. In Sudnow, D. (editor). Studies in Social Interaction, New York: Free Press.
SCHEGLOFF, E. A. (1992) 'Introduction'. In Lectures on Conversation, vol. 2, Harvey Sacks, ix. Cambridge, UK: Blackwell.
SCHEGLOFF, E A. (2006) '"Narrative Analysis" Thirty Years Later' in Atkinson, P and Delamont, S (editors) Narrative Methods: volume 1. London: Sage Publications Ltd
TILLY, C (1994), Big Structures, Large Processes, Huge Comparisons. Russell Sage Foundation: USA
TILLY, C (1999), 'The Trouble with Stories' in Pescosolidi, B.A. and Aminzades, R. (editors) The social worlds of higher education: handbook for teaching in a new century. Pine Force Press: California
WETHERELL, M and SCHEGLOFF, E. A. (1998) 'Positioning and interpretive repertoires: conversation analysis and post-structuralism in dialogue' Discourse and Society, 9(3): 387-416. [doi:10.1177/0957926598009003005]
WILKIE, P., MARKOVA, I., FORBES, C.D, and KENNEDY, A.C. (1985) 'Adult Polycystic Kidney Disease: A Study of Medical and Social Problems'. Health Bulletin, 43/2: 76-84.
